
Part 2: Can tech help in averting next winter crisis?

In the first article of two-part series, we reported how some of the global digital exemplars are using digital to address the demands on the health service.
In this second article, Shreshtha Trivedi looks at how primary care and urgent care sector are using digital to respond to these pressures, what is working and how can we accelerate the transformation agenda for next winter.
As acute trusts struggle to cope with wider problems facing the NHS and social care, it all comes back to oft-asked question: how can we keep patients out of hospital in the first instance?
The responsibility for this has been borne by general practitioners, NHS 111 and urgent care sector such as out-of-hours service providers.
Though the critics of NHS 111, the non-emergency telephone helpline offered by NHS England, say it exacerbates the problem by causing over-referrals to A&Es and increasing demands on ambulance service.
Former president of Royal College of Emergency Medicine, Dr Clifford Mann, had told the health select committee that more than 400,000 extra patients seen in A&Es the previous year had come via NHS 111.
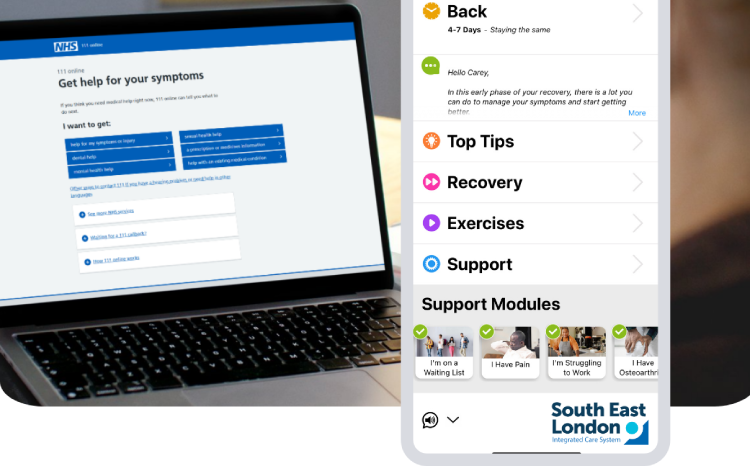
In addition to telephone support, other triage options include getting advice from NHS Choices portal and consulting local pharmacists
The burdens of winter pressures will continue so we need to look at how we are going to deal with it, argues Harry Longman, chief executive of GP Access.
“One answer could be looking at how do we make GPs more efficient.”
He says technology which enables GPs to message patients electronically and directing them to sites such as NHS Choices could help improve GP efficiency.
Another interesting trend has been the emergence of apps such as GP at Hand. Launched by digital health provider Babylon, it promises to cut waiting times by giving patients the option to video chat with their GPs.
And while it has been hailed for its “innovative” approach to general practice, it has also been accused of cherry-picking patients and contributing towards health inequalities.
Remote working
One of the key benefits of using these digital tools is the flexibility they offer.
Dr Taz Aldawoud. a GP and clinical board member at Bradford Districts Clinical Commissioning Group, thinks remote working can help in matching capacity with demand.
Aldawoud is also the creator of Doc Abode – a software platform providing quicker and effective healthcare solutions to NHS patients at home by increasing the availability and accessibility of local clinicians.
Supported by Yorkshire & Humber Academic Health Science Network, Doc Abode’s aims is to create a safer and more responsive urgent care system by using algorithms to match the skillset of the clinician with the specific needs of the patients.
Dr Aldawoud explains how it works: “When the core service is struggling, the provider pushes out a notification to those GPs who want to flexibly offer their time, and it’s up to the clinicians to set when they are available. If they are available at that time then they are notified of where the patient is, how far they are from the patients, other criteria which matches with their specialty, language etc and it’s up to that clinician whether to accept or reject that notification.”
He says the trial last year showed 15-20 percent of all urgent care activity was picked up by Doc Abode – which was independently evaluated by University of Bradford. In addition, the average time taken was under 30 minutes from the GP accepting the request to being face-to-face with the patient.
Cloud technology
Mark Cockerton has worked as a chief executive for three GP out-of-hours providers. A former advisor to Department of Health’s urgent care team, he argues that most people are aware of the long waits at A&Es in winter but they still choose that option because the alternative services aren’t as efficient as they could be.
The solution, he says, is to provide efficient and quick triage by using digital technologies such as the cloud. Pointing to a recent study by a cloud communications provider, he claims this flexible way of working helps in improving patient care as well as easing the strain on doctors.
“There is evidence out there that says you can bring flexibility and encourage people to access services over the phone if there isn’t an engaged tone, or if the call isn’t abandoned midway and if they don’t think they will have to wait to hear back.
“So if we could be slicker and give them a speedier response via cloud, then more people will phone in instead of walking into A&E.”
According to Cockerton, even though only half of the out-of-hours providers are currently using remote working in England, some of them are taking big strides. He gives example of GP out-of-hours initiative in Hackney to affirm that smaller, bespoke programmes catering to specific needs of the local population can make a difference.
“One of the issues we faced in Hackney was that out of 250,000 patients, about 40000 are Orthodox Jews who don’t access services during Sabbath. So the minute the Sabbath ends on Saturday, the service saw a spike in demand.
The solution was to get GPs dial-in from home on the cloud with a voice recorded system from any phone at all at the end of sabbath.
Cockerton believes if the GPs had gone to Homerton hospital at that time, it would have been a waste of resources and money. “Instead of a single GP spending five hours, if you can get 5 or 6 doctors doing an hour each when it gets very busy, then it’s a much better service for patients.”
Challenges and opportunities
Though the move towards digital way of working is not without its challenges. Aldawoud says clinicians are still not used to accessing all the information, including patient care records, on their smartphones.
While digital isn’t a silver bullet solution for all its problems, it can definitely help the NHS navigate the choppy waters of 21st century healthcare.
Technologies such as remote working, cloud, interactive portals and software have the potential to quickly and effectively address the needs of the patients while providing a flexible working environment for the clinicians. The key is to ensure the services are inclusive and not creating a two-tier system.
Whereas in the long run, data analytics will assist with predicting clinical outcomes, removing bottlenecks, and managing population health.
However, it is having a single, integrated digital care record across health and social care, that can have the biggest impact in alleviating winter pressures. Providing clinicians with access to access to extended patient data will help in filling the gaps in care and reducing pressure on hospitals.
NHS Digital understands its importance and if the health service can start implementing this, then maybe the next winter crisis can be averted.


5 Comments
Technology can help avert the next winter crisis but, as with any digital transformation project, it’s not as simple as just investing in the technology to unlock efficiency gains and new ways of operating. The NHS must also invest in changing the culture among those working in the health service to support their new ways of working with technology.
amen
The crisis that hits the media every 2nd of January is largely due to a failure to discharge patients from hospitals when staff in health and social care take their leave for the festive season. Anyone got an app for that?
PS if you think 111 telephone triage is bad, watch out for 111 digital. You couldn’t make this up – dissected here https://askmygp.uk/revealed-tiny-take-nhs111-digital/
Vital to distinguish between services which add to clinical costs by paying GPs outside of GMS, and those which are included in the normal GMS/PMS GP contract, or OOH contract. Commissioners will pay twice if they don’t get this. Worse, these services are much less efficient and lose continuity.
#DOI I run askmyGP, which is within the normal GP list based contract.
Comments are closed.